Biceps Tendonitis and its exercises
Biceps Tendonitis
Biceps tendonitis is inflammation of the tendon around the long head of the biceps muscle. Biceps tendinosis is caused by degeneration of the tendon from athletics requiring overhead motion or from the normal aging process.

Symptoms of Bicipital Tendonitis
Pain in moving the upper arm is a common symptoms of bicipital tendonitis.
Tenderness and pain in the shoulder
Snapping sound in the shoulder
Tenderness and pain in the shoulder
Snapping sound in the shoulder
Difficulty in lifting something, condition worsening with lifting.
Weakness
Feeling of warmth in the shoulder region
Redness.
Epidemiology of Bicipital Tendonitis
Bicipital Tendonitis is common amongst athletes, especially those, who are associated with sports like tennis, cricket, baseball, weightlifting, kayaking etc. In fact, wheelchair athletes, due to excessive use of hand movements can also have inflammation of the tendons causing the condition. It is also seen in older patients, where the condition is caused by degenerative tendinosis.
Causes of Bicipital Tendonitis
Overuse, repetitive and continuous usage of the biceps tendon can cause Bicipital tendonitis. Due to overuse, damaged cells of the tendons fail to repair themselves. The lack of time to recuperate leads to inflammation and causing bicipital tendonitis. The common causes of Bicipital Tendonitis are –
- Repetitive sports activities and frequent work activities. Athletes, who swim, throw or use racquets and swing, are mostly affected by bicipital tendonitis.
- If the shoulders are torn and wearied for years and have not had the time to heal, it can lead to bicipital tendonitis.
- When the collagen arrangement of the biceps tendons is disrupted, it can lead to inflammation of the tendons.
Rehabilitative Exercises
You may do these exercises right away. If any exercise increases your pain, stop doing it. Avoid overhead lifting while your tendon is healing. Some of most useful and valuable exercises to get recovery in biceps tendinitis are
Active elbow flexion and extension: Gently bring the palm of the hand on your injured side up toward your shoulder, bending your elbow as much as you can. Then straighten your elbow as far as you can. Repeat 15 times. Do 2 sets of 15

Biceps stretch: 
Stand facing a wall (about 6 inches, or 15 centimeters, away from the wall). Raise your injured arm out to your side and place the thumb side of your hand against the wall (palm down). Keep your arm straight. Rotate your body in the opposite direction of the raised arm until you feel a stretch in your biceps. Hold 15 seconds. Repeat 3 times.
Biceps curl:  Stand and hold a 5- to 8-pound weight in your hand. If you do not have a weight, use a soup can or hammer. Bend your elbow and bring your hand (palm up) toward your shoulder. Hold 5 seconds. Slowly straighten your arm and return to your starting position. Do 2 sets of 8 to 12.
Stand and hold a 5- to 8-pound weight in your hand. If you do not have a weight, use a soup can or hammer. Bend your elbow and bring your hand (palm up) toward your shoulder. Hold 5 seconds. Slowly straighten your arm and return to your starting position. Do 2 sets of 8 to 12.
Stand and hold a 5- to 8-pound weight in your hand. If you do not have a weight, use a soup can or hammer. Bend your elbow and bring your hand (palm up) toward your shoulder. Hold 5 seconds. Slowly straighten your arm and return to your starting position. Do 2 sets of 8 to 12.
Single-arm shoulder flexion:
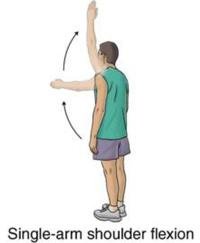
Stand with your injured arm hanging down at your side. Keeping your arm straight, bring your arm forward and up toward the ceiling. Hold this position for 5 seconds. Do 2 sets of 8 to 12. As this exercise becomes easier, add a weight.
Resisted shoulder internal rotation:
Stand sideways next to a door with your injured arm closest to the door. Tie a knot in the end of the tubing and shut the knot in the door at waist level. Hold the other end of the tubing with the hand of your injured arm. Bend the elbow of your injured arm 90 degrees. Keeping your elbow in at your side, rotate your forearm across your body and then slowly back to the starting position. Make sure you keep your forearm parallel to the floor. Do 2 sets of 8 to 12.
Resisted shoulder external rotation: 
Stand sideways next to a door with your injured arm farther from the door. Tie a knot in the end of the tubing and shut the knot in the door at waist level. Hold the other end of the tubing with the hand of your injured arm. Rest the hand of your injured arm across your stomach. Keeping your elbow in at your side, rotate your arm outward and away from your waist. Slowly return your arm to the starting position. Make sure you keep your elbow bent 90 degrees and your forearm parallel to the floor. Repeat 10 times. Build up to 2 sets of 15.
Side-lying external rotation:


Lie on your uninjured side with your injured arm at your side and your elbow bent 90 degrees. Keeping your elbow against your side, raise your forearm toward the ceiling and hold for 2 seconds. Slowly lower your arm. Do 2 sets of 15. You can start doing this exercise holding a soup can or light weight and gradually increase the weight as long as there is no pain.
Sleeper stretch:

Lie on your injured side with your hips and knees flexed and your arm straight out in front of you. Bend the elbow on your injured side to a right angle so that your fingers are pointing toward the ceiling. Then use your other hand to gently push your arm down toward the floor. Keep your shoulder blades lightly squeezed together as you do this exercise. Hold the stretch for 30 seconds. Repeat 3 times.






